LISTERINE® does not adversely affect either salivary or plaque pH
Importance of pH of the oral cavity
In the healthy state, saliva has a pH range of 6.7–7.4.1 A lower (more acidic) pH, below the critical value of 4.3–5, will favour demineralisation of the tooth, with (re)mineralisation occurring at higher pH levels.2
Dental erosion (‘acid erosion’) is the process of loss of dental hard tissue due to acid exposure without bacterial involvement. There are a number of ways in which the pH of the mouth can be reduced to allow erosion to occur. Erosion due to intrinsic factors occurs due to exposure to stomach contents due to vomiting, which has a number of causes including medical conditions e.g. GORD, drug side effects, psychological or eating disorders, alcoholism, and pregnancy. Extrinsic factors for acid exposure include occupational exposure to acidic gases, acidic medications, and lifestyle and dietary factors such as the consumption of acidic food and drink, such as cola, fruit juice, vinegar or acidic fruits.3
The cariogenic process likewise involves acid. Cariogenic bacteria lower the pH through the production of acids, in particular short-chain carboxylic acids such as lactate, acetate and propionate. These metabolic acids can diffuse through hard and soft tissues to produce a variety of biological effects in the pathogenesis of dental caries, gingivitis, and periodontitis.4
Hence it is important that products such as mouth rinses do not produce significant or sustained acidification of saliva or plaque.
Effect of LISTERINE® on salivary and plaque pH
A crossover, controlled study was conducted to determine the effect of LISTERINE® on the pH of saliva and dental plaque.5
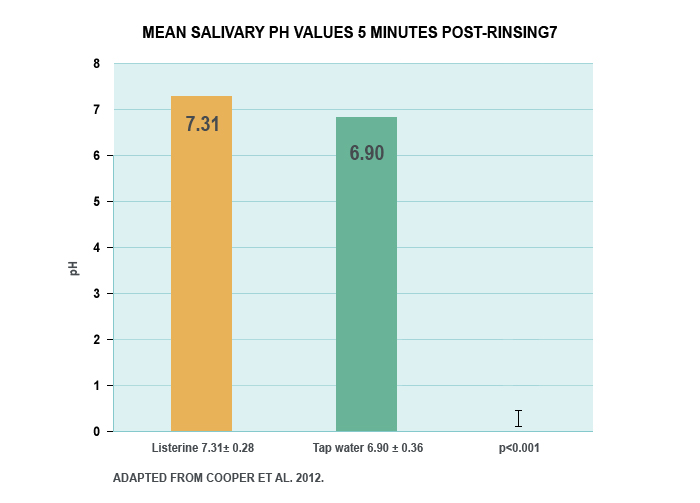
In this study, ten subjects rinsed with 20 ml of tap water for 30 seconds and salivary pH was determined at six time intervals up to 30 minutes. Ten minutes later the same subjects rinsed with 20 ml of LISTERINE® for 30 seconds and salivary pH was determined again. A second group of 10 subjects with 2 day old plaque rinsed with water and plaque pH was measured at the above intervals over 30 minutes. The same procedure was repeated with LISTERINE.5
LISTERINE® produced a significant increase in salivary pH through 5 minutes following rinsing compared with tap water (p<0.001).5
ph-body-image.jpg
After rinsing with LISTERINE®, both salivary and plaque pH remained well above pH 6 during the entire 30-minute period of the study. LISTERINE®’s low buffering capacity ensures pH returns rapidly to a level well above that required for acid erosion to take place.5
This study found that LISTERINE®, used as instructed, did not adversely affect the pH of saliva or dental plaque.5
Dental plaque contains oral bacteria that metabolise dietary fermentable carbohydrates to produce short-chain carboxylic acids such as lactate, acetate and propionate. These metabolic acids can diffuse through hard and soft tissues to produce a variety of biological effects in the pathogenesis of dental caries, gingivitis, and periodontitis. This clinical study evaluated the effect of rinsing with LISTERINE®, with or without fluoride, on plaque metabolic acid production and plaque pH response after a sucrose challenge.1
The aim of this in vivo study was to evaluate the effect of two antimicrobial mouth rinses on dental plaque acidogenicity after a sucrose challenge.1
References
Walsh LJ. Clinical aspects of salivary biology for the dental clinician. J Minim Interv Dent2008; 1: 7–24.
Arnold WH et al. Effect of pH of amine fluoride containing toothpastes on enamel remineralization in vitro. BMC Oral Health 2007; 7: 14.
Addy et al [eds]. Tooth wear and sensitivity. Informa Healthcare, London, 2000.
Zhang JZ et al. Effect of an essential oil mouthrinse, with and without fluoride, on plaque metabolic acid production and pH after a sucrose challenge. Caries Res 2004; 38: 537–541.
Steinberg L et al. Effects of an antiseptic mouthrinse on salivary and plaque pH. J Dent Res 1996; 75(IADR Abstracts): 3307.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
{* /socialRegistrationForm *}
Thank you for registering!
Register for LISTERINE® PROFESSIONAL
Stay up-to-date on all things LISTERINE®. Register today to receive relevant clinical information for your dental practice.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
Looks like you have an existing account with us. We have made some changes to our site and we need you to create a new password in order to login. Click send to recieve an email with instructions on how to create your new password.



Almost Done!
請在登入之前確認以下的資料。
{* #socialRegistrationForm *} {* socialRegistration_emailAddress *} {* socialRegistration_firstName *} {* socialRegistration_lastName *} {* socialRegistration_password *} {* socialRegistration_passwordConfirm *} {* socialRegistration_gender *} {* birthYear *} {* socialRegistration_addressStreetAddress1 *} {* socialRegistration_addressStreetAddress2 *} {* mobilePhone *} {* haveChildren *} {* customQuestions *}We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.