In a study from 2007, Kerr et al compared the effect of an alcohol-containing mouth rinse and a non-alcohol-containing mouth rinse on salivary flow and symptoms of dry mouth in healthy (non-xerostomic) adults.1
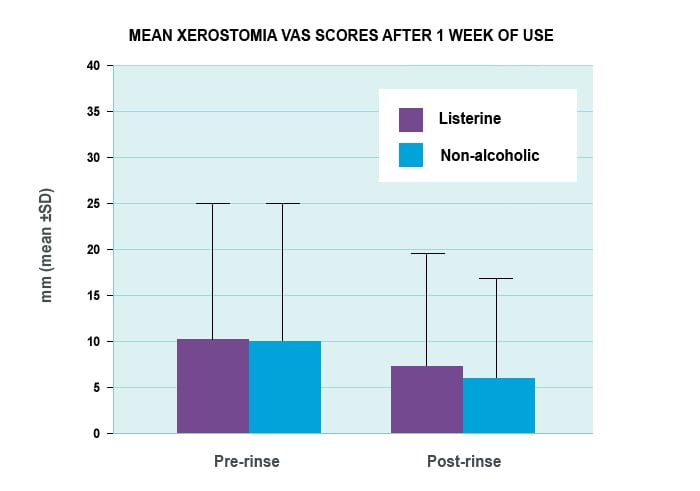
The observer-blinded, randomised, crossover pilot study involved 20 adults studied for 1 week. LISTERINE® was compared with a non alcohol-containing mouth rinse, 10 subjects per group. The subject rinsed with 20 ml of mouth rinse for 30 seconds; five minutes later whole salivary flow rates (ml/min) were determined. The subject’s subjective perceived mouth dryness was then ascertained on a 100 mm visual analogue scale (VAS).1
Mean xerostomia VAS scores after 1 week of mouth rinse use1
xerostomia-effect-body-image.jpg
Subjective perceived mouth dryness was ascertained by asking subjects to score on a 100mm visual analog scale (VAS) the "level of dry mouth you are experiencing now" (100 mm represented extreme dry mouth). The scale is a horizontal line and the patient marks on the line the point that they feel represents their perception of their current state.
No significant differences were found between the two mouth rinses in terms of salivary flow rate (p>0.05) or subjective sensations of dry mouth (p>0.05). In this study, the use of an alcohol-containing mouth rinse by non-xerostomic healthy adults did not increase the risk of xerostomia.1
Another study aimed to compare objective and subjective measures of dry mouth following extended (3 months) daily use of an alcohol-based mouth rinse, LISTERINE® Antiseptic, and a non-alcohol based mouth rinse, Crest® Pro-Health™ Rinse, on a population of healthy adults with ‘normal’ baseline salivary flow rates.2
This was a single site, randomised, observer-blinded, parallel designed study comparing the two mouth rinses to evaluate their impact on unstimulated whole salivary flow rates (primary objective outcome), and on perceived dryness (secondary subjective outcome) following daily use at weeks 4 and 12 versus baseline. Flow rates were measured in ml/min and perceived dryness was measured in millimeters on a visual analog scale (VAS) using a number of validated items and factors generated by the Bluestone Mouthfeel Questionnaire (BMQ). For the primary outcome, non-inferiority between-treatment comparisons (set at a margin of 0.15 ml/min) were made. For the secondary outcome, between-treatment comparisons of the mean BMQ VAS scores were made, with emphasis on item 2 (“my mouth feels dry”) and factor 2 (“cleanliness”). ANCOVA models were used to determine the significance of differences.2
One hundred and sixteen subjects successfully completed this study (n=60 Crest® Pro-Health™, n=56 LISTERINE® Antiseptic). The measures of dry mouth were comparable between the two mouth rinses, as demonstrated by non-inferiority of LISTERINE® versus Crest® Pro-Health™ with respect to salivary flow rates at both 4 and 12 weeks (p<0.001). Additionally, no significant differences between groups in the BMQ measures were observed at 4 or 12 weeks.2
Based on this study, extended daily use of an alcohol-based mouth rinse containing essential oils is no more likely to cause a reduction in salivary flow or perceived dryness than a non-alcohol based CPC mouth rinse.2
References
Kerr AR et al. A comparison of the effects of 2 commercially available nonprescription mouthrinses on salivary flow rates and xerostomia. Quintessence Int 2007; 38(8): e440–447.
Kerr AR et al. Comparison of two mouthrinses on salivary flow and perceived dryness. IADR General Session, San Diego, California, March 16-19, 2011. Abstract 784.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
{* /socialRegistrationForm *}
Thank you for registering!
Register for LISTERINE® PROFESSIONAL
Stay up-to-date on all things LISTERINE®. Register today to receive relevant clinical information for your dental practice.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
Looks like you have an existing account with us. We have made some changes to our site and we need you to create a new password in order to login. Click send to recieve an email with instructions on how to create your new password.

Almost Done!
請在登入之前確認以下的資料。
{* #socialRegistrationForm *} {* socialRegistration_emailAddress *} {* socialRegistration_firstName *} {* socialRegistration_lastName *} {* socialRegistration_password *} {* socialRegistration_passwordConfirm *} {* socialRegistration_gender *} {* birthYear *} {* socialRegistration_addressStreetAddress1 *} {* socialRegistration_addressStreetAddress2 *} {* mobilePhone *} {* haveChildren *} {* customQuestions *}We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.