Mouth rinse and its potential role in patients with dentine hypersensitivity
Dentine hypersensitivity
When in discussion with dental professionals, patients might complain of 'sensitive teeth'. There are a number of potential causes for this symptom, and the differential diagnosis should exclude other potential causes – cracked tooth syndrome, fractured restorations, chipped teeth, dental caries, gingival inflammation, post-restorative sensitivity, marginal leakage, pulpitis or palatogingival grooves – before dentine hypersensitivity is confirmed.1
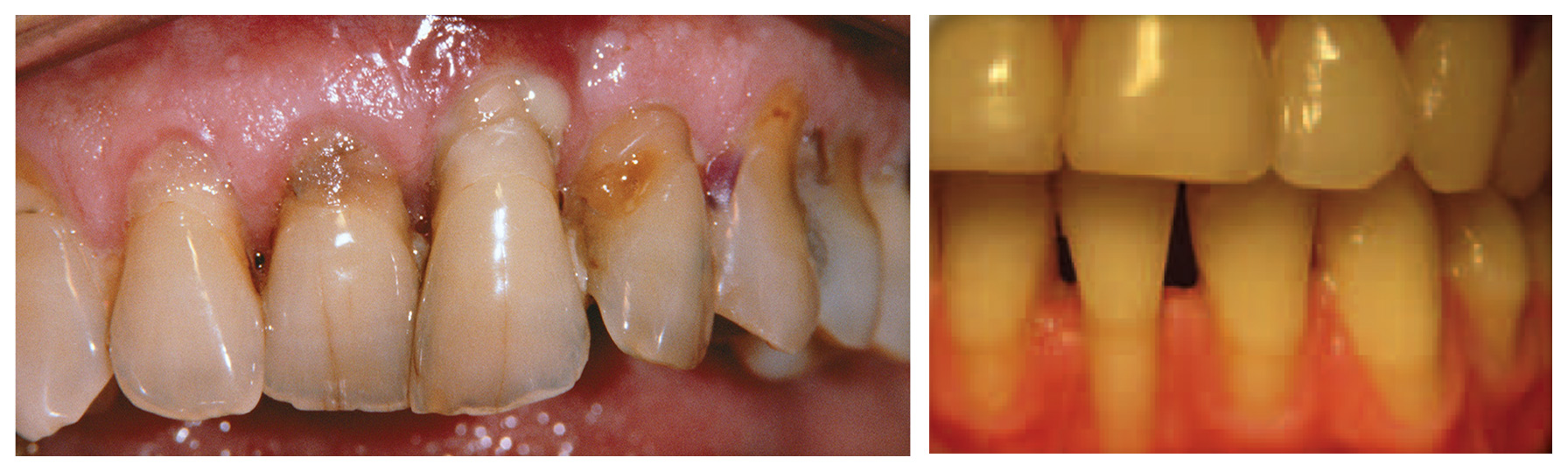
Dentine hypersensitivity, which has been defined as a 'short, sharp pain arising from exposed dentin in response to stimuli typically thermal, evaporative, tactile, osmotic or chemical and which cannot be ascribed to any other form of dental defect or pathology' has a number of potential causes, including gingival recession and tooth wear.1
Gingival recession is frequently the result of plaque-induced gum disease and/or excessive brushing. Tooth wear (attrition, abrasion, erosion, abfraction) can lead to exposure of dentine tubules.1
A long-term programme is often needed for this long-term problem, which may include dietary advice to tackle excessive consumption of acidic foods. Patients may also need advice on change of brushing technique/reduction in brushing frequency, or it may be beneficial to consider not brushing immediately after meals, but at a different time.1
Regular interdental cleaning may also be beneficial.
References
Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc 2003; 69(4): 221–226.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
{* /socialRegistrationForm *}
Thank you for registering!
Register for LISTERINE® PROFESSIONAL
Stay up-to-date on all things LISTERINE®. Register today to receive relevant clinical information for your dental practice.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.
Looks like you have an existing account with us. We have made some changes to our site and we need you to create a new password in order to login. Click send to recieve an email with instructions on how to create your new password.




Almost Done!
請在登入之前確認以下的資料。
{* #socialRegistrationForm *} {* socialRegistration_emailAddress *} {* socialRegistration_firstName *} {* socialRegistration_lastName *} {* socialRegistration_password *} {* socialRegistration_passwordConfirm *} {* socialRegistration_gender *} {* birthYear *} {* socialRegistration_addressStreetAddress1 *} {* socialRegistration_addressStreetAddress2 *} {* mobilePhone *} {* haveChildren *} {* customQuestions *}We collect your personal information to process your request to create an account for this web site. If you did not give us your personal information we would be unable to open your account. Your personal information will be processed and stored by our contracted service provider who supports this site on our behalf and they are located in the USA.
With your express consent, which you give us by registering and opening an account on our web site, we will send you exclusive offers, product updates and other promotional information about our product range by mail, SMS or email.You may revoke your consent to our use of your personal information at any time by telling us or updating your details on the site. Also, subject to exceptions permitted by applicable law you may request access to, or correction of, your personal information. For further information about how you might revoke your consent, request access to or correction of your personal information, make a privacy enquiry or complaint, or see our full Privacy Policy please<click here>
By pressing “Submit” you expressly consent to : * Receiving marketing communications from us by mail, email or sms; * Your personal information being processed and stored outside your country of residence; and * Your personal information being processed by our contracted service provider.